When you constantly feel dizzy and out-of-sorts with your daily activities, your whole world can seem upside down. Don’t wait to address your symptoms—it could be a simple to fix or something more serious.
As you read on, please know that we strongly recommended to see a healthcare professional to evaluate and diagnose the cause of your vertigo. Serious issues with the nervous system can lead to spinning, lightheadedness, and dizziness. It’s a good idea to have your doctor rule out any other condition before a physical therapy referral.
What is Vertigo?
Vertigo is a sense of dizziness or spinning that causes nausea and makes daily life difficult. It is a relatively common complaint, and prevalence increases with age.
Vertigo is often interchanged with a condition called benign paroxysmal positional vertigo (BPPV), although they are not the same. While BPPV is the most common cause of vertigo, not all vertigo is BPPV.
We will get into the other possible causes of vertigo, but let’s focus on BPPV first.
What is Benign Paroxysmal Positional Vertigo (BPPV)?
BPPV stands for Benign Paroxysmal Positional Vertigo. It is a sudden attack of dizziness or spinning that occurs with a specific head position. But what causes the dizziness to occur?
Imagine tiny crystal-like particles called otoconia. These particles are naturally found embedded in the membrane of the inner ear. Sometimes, the otoconia are displaced into the open fluid of the inner ear’s canals.
When you move your head, the free-floating otoconia will hit sensors in the canals, sending the brain some crazy messages: “The head is moving this way! Now that way! I’m confused!”
Now your brain thinks the head is moving more than it actually is, and your world will start to spin until the particle(s) settles. It can take a few seconds.
There are three canals that can be affected. The three canals are the posterior, anterior, and horizontal canals. Some canals are more commonly affected than others. For instance, about 90% of cases are in the posterior canal, about 9% in the horizontal canal and the last 1% in the anterior canal. (3)
You would need to get the condition assessed by a physical therapist before you know which canal is affected. Thankfully, there is treatment for all of them!
Be assured that no permanent damage is caused by BPPV. It can be a quick fix, although recurrences could happen. About 40% of people with BPPV have had it before. (2)
There is no permanent cure, but the treatment is extremely effective and can stave off vertigo for months to years.
Symptoms of BPPV

Spinning and imbalance are primary indicators of BPPV. The symptoms will occur with specific positional movements and range from low to high intensity. Spinning usually lasts less than 15 seconds, but in rare cases, it can linger for almost a minute.
During your episode, you will likely experience rapid involuntary eye movement called nystagmus. This occurs because your eyes are getting mixed signals and they’re trying to catch up, so your eyes vibrate in certain patterns until the condition settles down.
Here are some common aggravating movements, although everyone is unique:
- Rolling over in bed
- Bending over
- Standing up from couch or bed
- Putting in eye drops
- Sitting in a dental chair
It is 40% more common to get BPPV in the right ear than the left. (4) It is also more common to develop symptoms on the side you sleep. In fact, some people are able to lessen the frequency of their BPPV by sleeping on the other side.
Who Can Develop BPPV?
There are several risk factors. Age and gender are the major ones.
Females are twice as likely as males to get BPPV. This could be due to accelerated bone degeneration in women. The fragments can end up in the canals obstructing the fluid and therefore causing the vertigo. (1)
Of those who experience BPPV, 97% are over 40 years old and 10% are over 75 years old. (1) Those with osteoporosis or history of head trauma have a higher likelihood of developing BPPV. There is also a genetic predisposition, so if your grandmother has it, you have a higher chance of developing it too.
How is BPPV Treated?

It is important to note that there are many possible causes of dizziness and vertigo. A trained physical therapist who specializes in vestibular disorders should provide a complete assessment to rule out other causes.
However, if BPPV is diagnosed, your chance of a full recovery is good. You will need between one to three visits involving canalith repositioning, follow-up education, and some homework.
Canalith repositioning techniques are implemented by a trained physical therapist to remove the loose particles in the canals and restore normal fluid movement. These techniques are relatively comfortable and calm, although it’s normal to feel some symptoms as the otoconia are guided out of the canals. Treatment is non-invasive, easy, and quick.
But remember: BPPV is treated but not cured. It can return. There is a 25% chance that the symptoms will return within a year, and a 50% chance that they will return in 5 years. (3) However, your physical therapist will ensure that you understand your symptoms and are able to manage them if they do return.
Sleeping with BPPV

After a physical therapy session, you’ll know which ear is likely affected. To help reduce the frequency and intensity of BPPV at night or in the morning, you should sleep on the unaffected ear. In some rare cases, both ears may be affected, in which case you and your physical therapist will need to determine the best approach to sleep management.
After treatment using canalith repositioning maneuvers, it was previously recommended that patients with BPPV should sleep upright to help reduce the incidence of vertigo. (4) However, more recent research has shown that is not necessary. There may be an increased efficacy of 20% to sleep with the head inclined up 20 degrees or more, but it may not be worth the trouble. (4) Speak with your physical therapist concerning his/her recommendation for you.
Meniere’s Disease vs BPPV
If you’ve tried to self-diagnose on Google and WebMD, you may have seen Meniere’s disease a few times… and you’ve read about it… and now you’re panicking. Don’t panic!
Meniere’s disease is frequently confused with BPPV. Many decades ago, Meniere’s was used to describe most conditions with vertigo until further research revealed key differences in treatment and management.
Meniere’s is the most well-known unstable peripheral disorder of the vestibular system. It is difficult to treat. Only 1% of the population have it, and it is equally likely in men and women. Meniere’s is most common in middle-aged populations of European descent. This condition is very rare among those older than 60. (5)
The etiology is unknown, but there are genetic predispositions and autoimmune factors.
If you take away anything, take this… you probably don’t have it. Still unsure? Read ahead.
What are Symptoms of Meniere’s Disease?
Meniere’s disease causes intermittent spontaneous episodes of vertigo lasting 20 minutes to 2 hours. These episodes of vertigo will usually last for about seven years before the ear stabilizes by losing all of its vestibular input.
Patients will note a sense of fullness in their ears and accompanying tinnitus, which is ringing in the ears that begins intermittently and becomes constant until complete hearing loss. It takes 7-10 years to lose your hearing from Meniere’s.
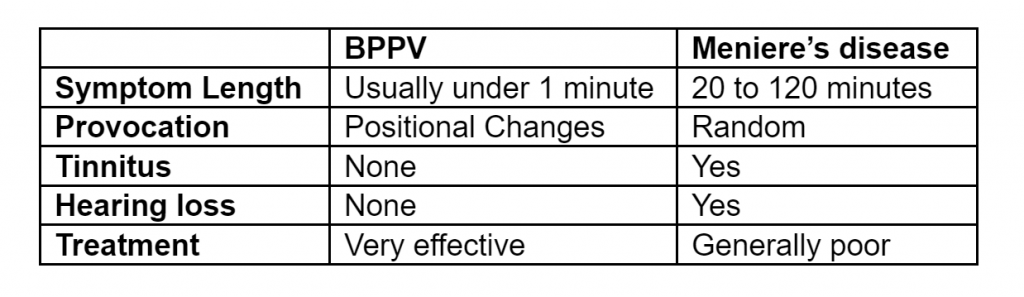
If you don’t have ringing in your ears and your dizziness only comes in short, predictable spurts… you likely don’t have Meniere’s. Take a look at this chart so you can compare your symptoms.
Treatment for Meniere’s Disease
In the small chance that you do have Meniere’s disease, still don’t panic.
Although there are no cures for Meniere’s, there are some management techniques.
Some doctors recommend reducing sodium intake. A few MDs may recommend diuretics or steroids. Others will recommend a last-resort injection which has some gnarly after-effects, which can be managed with physical therapy later.
If your diagnosis is 100%, undeniably, certainly, without-a-doubt Meniere’s Disease, then your doctor will discuss treatment options.
What About Vestibular Hypofunction?
Vestibular hypofunction is a treatable category of disorders and is associated with vertigo, which can last for days to a week.
Some common symptoms of vestibular hypofunction are nystagmus and double vision caused by head movement with no relief with rest, unlike BPPV.
The recovery process, while effective, does take a little longer than BPPV. It can take about 1-2 months for complete resolution versus 1-2 weeks for BPPV. A complete recovery is very possible with the use of adaptation exercises.
There are two types of hypofunction disorders: stable and unstable. Stable hypofunction can be treated with physical therapy. Unstable hypofunction requires medical intervention.
Some Examples of Stable Hypofunction:
- Vestibular Neuritis: Vestibular neuritis is typically a one-time event lasting days that is caused by herpes simplex virus. A patient might have had a respiratory or GI infection before these symptoms began. The virus affects the superior vestibular nerve which innervates the anterior and horizontal canals. Corticosteroids could help manage the symptoms.
- Anterior Vestibular Artery Ischemia: Anterior Vestibular Artery Ischemia is another possible cause of vertigo. It refers to a lack of oxygen to the anterior vestibular artery. This is often seen in individuals with certain cardiovascular risk factors like diabetes, smoking, atrial fibrillation, hypertension, prior history of strokes, obesity, or tobacco use. Medical management focuses on reducing these risk factors.
- Labyrinthitis: Labyrinthitis is inflammation of the inner ear’s labyrinth. It is caused by a virus and could cause unilateral hearing loss and tinnitus if not treated. The medical treatment is oral or transtympanic corticosteroids (in the ear) to reduce inflammation until the body fights off the virus.
Some Examples of Unstable Hypofunction:
See your doctor for treatment options as physical therapy is not the first-line treatment approach.
- Meniere’s Disease
- Otolithic Crisis Events of Tumarkin
- Acoustic Neuroma / Vestibular Schwannoma
- Anterior/Superior Canal Dehiscence (ACD)
What are Exercises for Vertigo?



There are various approaches to vertigo treatment depending on your diagnosis:
- BPPV is treated with canalith repositioning maneuvers. Certain canalith repositioning maneuvers are used depending on the affected canal. Some common techniques are the dix-hallpike maneuver for the posterior canal and the supine or BBQ roll test for horizontal canal.
- Gaze instability is treated with gaze stabilization exercises. Gaze stabilization can help with oscillopsia which is blurred vision due to abnormal eye muscle coordination. One of the best approaches is to address the vestibular ocular reflex with exercises explained and dosed by your therapist. The exercises can be progressed or regressed to find the right level of challenge for you.
- Peripheral hypofunction is treated with habituation exercises. Habituation exercises can help decrease symptoms aggravated by rapid head movements or busy environments. Habituation exercises work by desensitizing the vestibular system to these stimuli. When prescribed by a physical therapist, these exercises can be quite effective, but you must do them consistently.
- Balance deficits can be improved with balance training. Balance exercises will help enhance your body’s use of sensory input to decrease the chance of a stumble or fall as a result of your condition. The vestibular system works with your seeing and feeling senses to maintain balance.
Without the ability to see (ex. if it’s dark) or feel (ex. neuropathy of the feet), your vestibular system has to work harder. Training balance in different conditions allows you to reduce dependency on visual or tactile information for whatever life throws at you.
Talk to your therapist to see which balance exercises are appropriately challenging for your condition, and if it’s safe for you to practice them at home.
FAQs
Can Temporomandibular Dysfunction (TMD) cause vertigo?
No, these are two conditions that often coincide. However, TMD can also be treated by a trained physical therapist.
What are some alternative causes of vertigo?
If you’re stuck, look into these alternative diagnoses. If your symptoms are evolving, tell your doctor as alternative diagnoses can become more likely – and can be serious.
- Migraine Positional Vertigo
- Cerebellar Dysfunction
- Multiple Sclerosis
- Orthostatic Hypotension
- Cerebellar Pontine Angle Infarct or Tumor
- Chiari Malformation
Have more questions?
Call JACO Rehab and learn how to book an appointment with a physical therapist today!
Written by Nelson Almeida, DPT
Sources
1. Gizzi M, Ayyagari S, Khattar V. The familial incidence of benign paroxysmal positional vertigo. Acta Otolaryngological (Stockh ), 118:774-777, 1998
2. Helminski JO. Effectiveness of the canalith repositioning procedure in the treatment of benign paroxysmal positional vertigo. Phys Ther. 2014 Oct;94(10):1373-82.
3. Noda K, Ikusaka M, Ohira Y, Takada T, Tsukamoto T. Predictors for benign paroxysmal positional vertigo with positive Dix-Hallpike test. Int J Gen Med. 2011;4:809-14.
4. Shim DB, Kim JH, Park KC, Song MH, Park HJ. Correlation between the head-lying side during sleep and the affected side by benign paroxysmal positional vertigo involving the posterior or horizontal semicircular canal. Laryngoscope. 2012 Apr;122(4):873-6.
5. Wladislavosky-Waserman P, Facer GW, Mokri B, Kurland LT. Meniere’s disease: a 30-year epidemiologic and clinical study in Rochester, Mn, 1951-1980. Laryngoscope. 1984 Aug;94(8):1098-102.