
Have you ever felt a “pinch” in the front of your hip when you squat?
Maybe you were trying to put on your shoes and the hip felt “stuck” or “locked”.
Locking, pinching, or stiffness felt in the groin or hip can sometimes be due to a lack of space in the joint. One common reason is a bony overgrowth either on the head of the thigh bone or its socket.
This condition is commonly referred to as Femoral Acetabular Impingement or FAI.
Let’s take a closer look at FAI and how it may be the cause of your hip pain and stiffness.
Hip Anatomy
The hip is made up of two bony surfaces. The femur, or thigh bone, and the acetabulum, or socket.
-

- The femur (highlighted) is part of the hip joint | Image courtesy of Complete Anatomy
The femur sits deep into the acetabulum thanks to the acetabular labrum, cartilage that increases the depth of the joint by 21%. The labrum also provides a vacuum-like seal to help maintain hip stability in conjunction with the ligaments of the hip joint. It also acts as a cushion for the bony surfaces to prevent them from rubbing together.
The labrum is helpful in protecting soft tissues of the hip from injury, including the muscles and ligaments, by transmitting force throughout the joint. It increases the overall surface area of the joint by 28%.
-

- The labrum of the hip | | Image courtesy of Complete Anatomy
When bony overgrowth of the head of the femur or acetabulum occurs as in FAI, this can lead to breakdown of the acetabular labrum, which in turn can lead to pain and overall movement dysfunction. If FAI is left untreated it can lead to premature osteoarthritis and joint stiffness affecting your ability to squat, sit, and participate in sports.
The Two Types of FAI
FAI can affect both the femur and the acetabulum together or separately referred to as a Cam, Pincer, or Combined lesion, respectively.
A Cam lesion refers to bony overgrowth of the neck of the femur resulting in loss of space for the femur to slide within the acetabulum. Typically, this will limit the ability of the hip joint to flex (such as in bringing your knee to your chest). This limitation causes pain with squatting, sitting, or other sport-specific activities like running, dancing, or gymnastics.
A Pincer lesion refers to bony overgrowth of the acetabulum resulting in a deeper socket of the hip joint. This then alters the normal mechanics of the joint causing a loss of general range of motion, specifically of extension (kicking the leg back), abduction (kicking the leg out to the side), and internal rotation (turning foot outwards with the knee bent/crossing your legs).
Typically, both types of FAI are first treated by non-surgical means including – you guessed it – physical therapy! In conjunction with physical therapy, oral steroids or steroid injections, and/or activity modification may be required to manage your symptoms.
Some lesions may require surgical intervention to correct. Commonly, hip arthroscopy is done to shave down the bony overgrowth and debride or repair the damage done to the acetabular labrum. In severe cases of FAI, a total hip replacement may be required to correct the damage.
In order to determine what course of treatment is right for you, follow-up with your primary care physician or an orthopaedist who specializes in treating hip dysfunction. An orthopedic specialist can usually take an x-ray and/or MRI to determine the type of lesion you have, amount of damage to the labrum, and the amount of arthritis that may be present. Your orthopaedist can then determine the best course of action for treating and managing your symptoms.
What Causes FAI?
The cause of FAI is not well known, but most research suggests a familial link with improper bone development in childhood being the major contributing factor.
Exercise alone cannot cause FAI, but with repetitive trauma to the hip as in contact sports, or improper mechanics with jumping, cutting, or running, the pain and disability associated with FAI can occur more quickly.
Ensuring safe tackling techniques while playing contact sports, learning how to jump and land safely, and learning proper lifting/running mechanics can help to delay the onset of FAI.
If you are an athlete looking to improve your form or prevent hip related injuries including FAI and labral tears, contact our JACO Kapolei office at (808) 381 – 8947 for a sports and injury prevention assessment!
Physical Therapy for FAI
Physical therapy for FAI initially involves decreasing and managing any swelling or pain and restoring normal range of motion at the hip joint.
Typically, joint mobility, stretching, strengthening of the hip can resolve some stiffness and general pain.
Commonly tight and weak muscles of the hip include the following:
- The iliopsoas or major hip flexor (think bringing your knee to chest)
- The gluteus medius or major hip abductor (think bringing your leg out to the side)
- The piriformis or major hip external rotator (think putting on your shoes and socks)
The Iiliopsoas
The iliopsoas muscle is made up of two separate muscle bellies, the iliacus and the psoas.
The psoas muscle actually originates at the upper lumbar spine, or low back, and then crosses at the hip where it attaches to the greater trochanter of the femur.
-
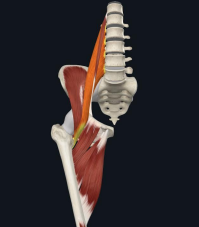
- Iliopsoas | Image courtesy of Complete Anatomy
Because it crosses at the low back, if this muscle is tight, it can cause the back to arch thereby limiting the ability of the glute max to contact and hip to extend further exacerbating stiffness caused by FAI.
The Gluteus Medius
The gluteus medius runs from the ilium or pelvic bone again to the greater trochanter of the femur. The backside of the muscle sits beneath the large glute max. The frontside of the muscle is primarily covered by a thick fascial band that connects with the quadratus lumborum muscle of the back and iliotibial band of the thigh. Because the front portion is covered by this tick fascial layer, it can be tough to stretch and lengthen!
-

- Gluteus Medius | Image courtesy of Complete Anatomy
The gluteus medius is an interesting muscle in that it pretty much moves the hip in every direction, although it is primarily a hip abductor (think bringing the leg out to the side and getting into/out of the tub or car).
The front fibers of the gluteus medius also flexes and internally rotates the hip, while the back fibers extend and externally rotate the hip.
When the hip is flexed to about 90 degrees (think while sitting), the glute medius will internally rotate the hip eight times what it normally does! A prolonged internally-rotated hip position can feel uncomfortable. So, if the gluteus medius is tight causing internal rotation of the hip, it can be the culprit responsible for that “pinchy” sensation.
The glute medius is also a very important muscle for walking, running, and single-leg activities as it prevents the opposite hip from dropping and provides a great deal of stability to the hip. Loss of strength of this muscle can and frequently does result in other issues such as knee, foot, and ankle pain.
The Piriformis
We commonly hear about the piriformis muscle when someone thinks they have “sciatica”. This is because the long sciatic nerve usually runs underneath this muscle. If it’s tight, it can impinge the nerve resulting in radiating pain into the foot or toes.
The muscle originates from the sacrum and attaches again to the greater trochanter. The piriformis muscle is responsible for externally rotating the hip. This keeps the hip joint space open and allow for easier sitting, squatting, and walking/running.
-

- Piriformis | Image courtesy of Complete Anatomy
Physical therapists will typically perform soft tissue mobilization including trigger point release or active tissue release to these muscles as well as joint mobilizations to improve your range of motion.
Once normal range of motion is restored, your physical therapist will develop an individualized exercise program for you to work on stretching and/or strengthening of the muscles of the hip and pelvis, including the core, depending upon the muscle dysfunction.
Ultimately, this combination of manual treatment and exercise prescription is what will get you back to daily functioning without pain and the things you love doing!
Two Exercise Examples for FAI
Hip Flexor Stretch

- Grab a chair/stool and place the opposite leg up on it. Make sure your knee stays in line with your second and third toe to prevent any pinching in the hip or groin. If you are worried about balance, grab a second chair to hold on to for safety. Or, perform the stretch next to a counter.
- Make sure the leg you are trying to stretch is far enough behind you and your toes are pointed straight ahead.
- Tighten your core and glutes by pulling your belly button to the spine and clenching your butt cheeks together during an exhale.
- Hold the stretch 3 times for at least 30 seconds. You should feel it in the front of the standing leg.
Hip Abductor Strengthening

- Stand at your kitchen counter or hold onto a chair for balance.
- Tighten your glutes by squeezing or clenching your butt cheeks together.
- Lock your knee.
- Lift the opposite leg out to the side ensuring your toes are pointed forward. Standing up tall, and your hips are not “hiking” up.
- Perform 3 sets x15 repetitions on each side. You should not feel this exercise in your back!
To increase the challenge of this exercise…
- Lay on your side with your back against a wall.
- Tighten your glutes by pinching/clenching your butt cheeks together.
- Slide your heel up the wall ensuring your toes are pointed forward.
- Keep a hand on your hip to ensure you do not “hike” it up by using your trunk.
- You should feel this exercise along your buttock region.
Need Some Help?
Visit JACO Rehab for guidance in your rehabilitation journey. We have four locations on Oahu including Honolulu, Kapolei, Waikele, and Mililani. Most locations are open seven days per week with early and late appointment slots to accommodate your busy schedule. Reach out – we can help!